August 2019 Newsletter
Mothers Are Dying. Mental Health Providers Can Help.
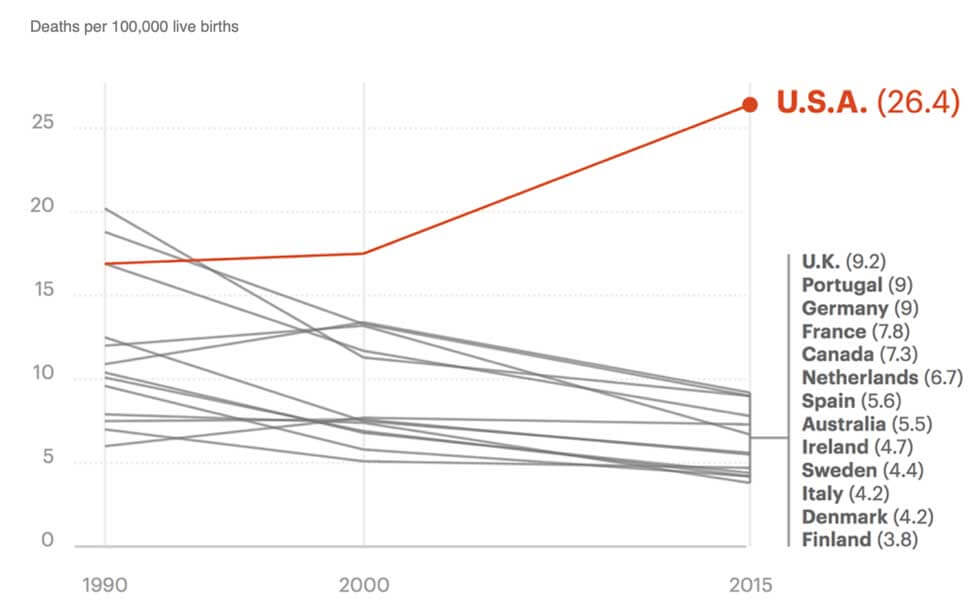
“Global, regional, and national levels of maternal mortality, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015,” The Lancet.
Last Tuesday, Melinda Gates launched her viral campaign, Equality Can’t Wait, in the hopes of shortening the timeline to gender parity in the United States.
With endorsements from celebrities and politicians alike, her new campaign is based on the latest Global Gender Gap Report which predicted that at our current rate, Americans will take 208 years to achieve gender equality.
Women’s health and survival rates comprise one of four categories used to assess gender-based disparity.
The current state of women’s health in the U.S. is life-threatening:
- More women are dying of pregnancy-related complications in the U.S. than any other developed country
- Of all medical complications affecting women during pregnancy, perinatal mood and anxiety disorders are the most common
- Suicide is a leading cause of perinatal maternal death
Mental Health Providers Can Help:
Understand root causes
Addressing barriers to maternal mental healthcare access is essential to an equitable future. Stigma, poor awareness, and teratogenic psychiatric medications make mental health treatment decisions for pregnant and breastfeeding women complex. Growing evidence suggests this complexity leads to treatment avoidance.
However, increased patient and provider education about nonpharmacologic treatment options for depression during pregnancy and breast-feeding may help reduce barriers to maternal mental healthcare access and utilization.
Educate yourself and others
In addition to standard mood disorder medications and therapies, repetitive transcranial magnetic stimulation (rTMS) is an effective, non-systemic and non-invasive treatment option for depression. Although rTMS is not FDA indicated for use during pregnancy, current evidence of rTMS for depression during pregnancy is encouraging.
rTMS, applied during the 2nd and 3rd trimesters of pregnancy, does not appear to cause any adverse birth outcomes. In sham controlled TMS studies conducted during pregnancy, no differences in cognitive or motor development between infants in active and control groups have been reported.
Start the conversation
Gender equality can start with a conversation, and this tool can help. rTMS is a promising treatment option for perinatal mood disorders and could significantly improve access and utilization of essential maternal mental health services during an important time for women and their families.
Believe it or Not!?
Health Hystory
Hippocrates, after observing what he described as the dreaded female ailment of excessive emotion, postulated that it must be caused by a displaced or “wandering uterus”. We’ve heard of a wandering eye, but this?
He named the ailment ‘hysteria’ after the Greek word, hysterika, or ‘uterus’. It’s root word, hyster-, can be found in many words used today. Isn’t that hysterical?
An Exclusive Q&A with Dr. Martha Koo, M.D.:
-
Are there any medical risks associated with untreated mood disorders during pregnancy?
On one hand, the choice to receive medical treatment during pregnancy is always a challenging decision for expectant parents.
On the other hand, we know that untreated depression during pregnancy is a risk for pre-term birth and low birth weight. Research also demonstrates that pregnant women with depression are at higher risk for poor self-care, pre-eclampsia, postpartum depression and suicidality.
Longitudinal studies document that maternal depression affects childhood development, leaving children vulnerable to cognitive, behavioral and emotional difficulties.
-
Why is maternal mental health such a challenging problem to tackle?
Mental health, in general, is challenging medically as there remains significant stigma in society surrounding mental illness. Maternal mental health is up against the additional societal idealization of motherhood– that women should be glowing during pregnancy and thrilled after birth.
This idealization contributes to the shame and secrecy I encounter in women struggling with depression and anxiety during pregnancy and postpartum. As society and providers become more educated, I hope stigma will diminish and access to treatment will improve.
-
What has been your experience treating pregnant women with rTMS?
At the Neuro Wellness Spa, I’ve had the privilege of treating many women during their pregnancies. It’s been surprising how supportive of rTMS their treating obstetricians have been.
Similar to what has been documented in clinical studies, none of my patients suffered any adverse maternal or infant outcomes, and all experienced mood improvement and reduced anxiety.
Where We’ve Been…

Mental Health Meetup at Tin Roof Bistro
From left to right: Marina Braff, LMFT, Jenny Moon, LCSW, Dr. Jillian Pexa, PsyD, Dr. Nazanin Moali, PhD, and Kathleen Ballue, Clinical Outreach for Discovery Mood & Anxiety Program

Perinatal Mental Health Brunch at Crème de la Crepe
From left to right: Abby Withee, LMFT, Christina Kalzadilla, LMFT, Dr. Martha Koo, M.D., Bryana Kappa, LMFT, Vi Ballard, LMFT, Evy Jacobson, AMFT, Marina Braff, LMFT, and Emily Pedersen, MPH, M.S.Ed
…Where We’re Going
2nd International Conference on Addiction Therapy & Clinical Reports
When : August 22-23, 2019
Where : Barcelona, Spain
What : Martha Koo, M.D. is a plenary speaker and will be giving a presentation on transcranial magnetic stimulation in the treatment of addiction.
We’re more than a newsletter. We give tours, offer consultations and can even speak at your event.
What Our Patients Are Saying
-
My Life Started To Turn Around

I had a very positive experience with Neuro Wellness Spa and would recommend them for TMS treatment. The psychiatrists and especially the technicians explained things to me clearly and had great bedside manner throughout my multi-week treatment. I had great results and am forever grateful!
Leah -
TMS therapy had a profound impact in a short period of time
I had an incredible experience with my TMS treatment. I felt appreciated and welcomed by the staff and my needs were met throughout the whole process. I was consistently checked on by the psychiatrist to assess progress. The technicians made me feel as comfortable as possible and I began to notice cognitive and behavioral differences after a short period of time.
Ramsey -
Mental health support backed by science
Neuro Wellness Spa is an amazing facility filled with excellent doctors, wonderful technicians and therapists, and cutting edge therapies. The Psychiatrists there are grounded in science and don’t just prescribe medications to help with mental health issues. They take the time to listen and tune into individual patient needs and prescribe a plan to fit those needs. I Highly recommend for anyone searching more holistic therapies.
Nancy -
Helped my depression and anxiety
Amazing staff and very helpful they have helped my depression and anxiety immensely highly recommend their services
Amber -
Got The RIGHT Meds
Spent decades on mental health medications that weren’t right for me. Took the genetic test, learned about what would work for me and got the RIGHT meds. Has made such a difference for me.
Jean -
TMS Changed Everything
I was so low on energy and TMS changed everything. Now, I look forward to starting my days. My focus has improved. I appreciate things I couldn’t even notice before.
Rob -
Full service support
I can’t say enough about the genuine quality of care and professionalism of all the psychiatrists and the TMS team have provided to our loved one! They truly care about each individual! Highly recommend!!
Robin -
TMS helped with my sleep
I underwent TMS maybe a year ago, and albeit I had only undergone it once, I had felt better about my day and definitely my nights, for it had benefited my sleep a lot. I found myself to be less anxious and less depressed as the process had carried on and found it to be an enjoyable experience overall.
Bryce

-

LGBTQ Youth Mental Health: Barriers to Care, Identity Formation, and Age-Appropriate Treatment
We are in an LGBTQ youth mental health crisis.1 According to a 2024 Nationa
-
Supporting Los Angeles Through Community Crisis
The recent challenges across Los Angeles — from devastating wildfires to heightened ICE enforcement a
-
Anxiety in Men: How Symptoms Differ, Overcoming Stigma, and Male-Focused Treatment
Anxiety is a mental health concern that people experience at varying levels of severity. Some people wi
-
Perinatal Depression: Q&A With a Psychiatrist
Pregnancy and becoming a new parent can bring profound joy, but it also triggers significant physiologi
-
How To Help Someone With OCD: 9 Evidence-Based Support Strategies
Watching a loved one battle obsessive-compulsive disorder (
-
PTSD Treatment: Q&A With a PMHNP
Approximately 7% to 8% of people will experience post-traumatic stress disorder (PTSD) at some time in
-
CBT for ADHD: Cognitive Restructuring Exercises Adapted for ADHD Treatment
In recent years, we’ve seen a dramatic and steady rise in
-
CBT for Depression: Restructuring Negative Thoughts
The impact of depression on your daily
-
Is Online Therapy Effective? Mental Health Solutions for Digital Platforms
Online therapy has steadily increased in popularity, especially since the
-
CBT for Anxiety: Cognitive Behavioral Therapy Techniques for Anxiety Disorders
If you’re struggling with anxiety, the pr